Population health management (PHM) strategies help organizations achieve sustainable outcomes improvement by guiding transformation across the continuum of care, versus focusing improvement resources on limited populations and acute care. Because population health comprises the complete picture of individual and population health (health behaviors, clinical care social and economic factors, and the physical environment), health systems can use PHM strategies to ensure that improvement initiatives comprehensively impact healthcare delivery.
Organizations can leverage four PHM strategies to achieve sustainable improvement:
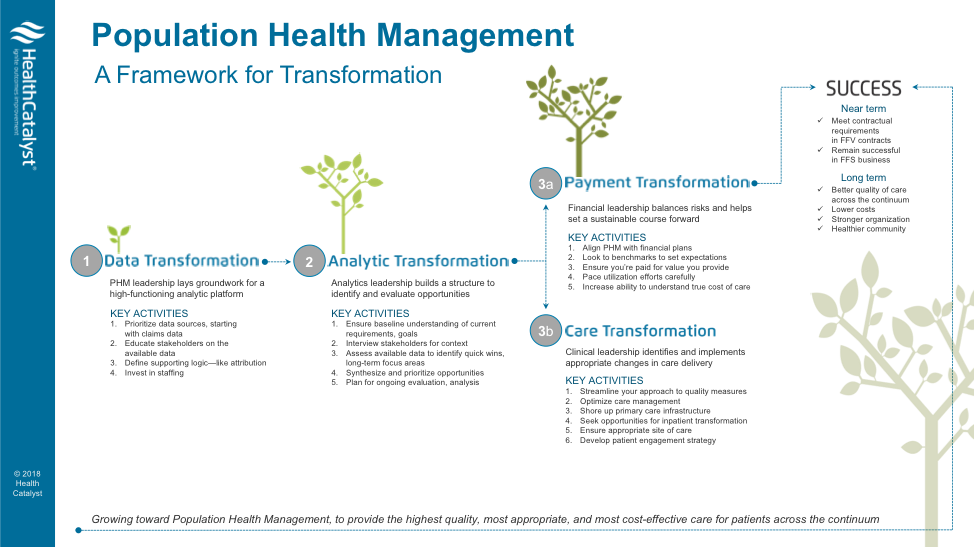
1. Data transformation
2. Analytic transformation
3. Payment transformation
4. Care transformation
 Download
Download
Population health management (PHM) strives to achieve IHI’s Triple Aim, including better outcomes for individuals across communities. Health systems working to improve healthcare outcomes can meet their goals by aligning improvement and PHM strategies. This article describes how organizations can use four PHM strategies to transform their approaches to data, analytics, payment, and care to improve outcomes and achieve sustainable change.
While many organizations define population health slightly differently, its core aim is to improving health outcomes of individuals and populations while improving efficiencies and reducing the total costs. IHI references a definition from population health researcher David Kindig: “Population health is defined as the health outcomes of a group of individuals, including the distribution of such outcomes within the group.” Kindig explains that populations “are often geographic populations such as nations or communities, but can also be other groups such as employees, ethnic groups, disabled persons, prisoners, or any other defined group.”
Regardless of how organizations define population strategies, PHM involves collaboration between leaders in healthcare, politics, charity, education, and business. Factors that make up the complete picture of individual and population health (Figure 1) span health behaviors (e.g., tobacco use, diet and exercise, and alcohol and drug use), clinical care (e.g., access to care and quality of care), social and economic factors (e.g., education, income, and family and social support), and the physical environment (e.g., air and water quality and housing and transit).
There are four PHM strategies organizations can use (Figure 2) to improve outcomes:
Organizations must be able to prioritize and integrate a multitude of internal and external data sources to provide better transparency into the population health journey. This transparency helps organizations better manage their networks, risks, opportunities, and strategies to efficiently improve health. The team working on the Alberta Health Services population health initiative concluded that only eight percent of the data needed for precision medicine and population health resides in today’s EHRs. This highlights the need to incorporate not only clinical data, but also data related to health behaviors, social and economic data, physical environmental data, claims data, cost data, engagement data, and a variety of additional sources. Practically speaking, this data can provide critical direction on ensuring delivery of the right services at the right time in the right place.
Once organizations have the right data to identify and evaluate opportunities for population health and improvement work, they will need an analytic structure that can deliver several key capabilities:
Organizations must transform their fee-for-service payment models to better understand the total cost of care and to balance the risk health that systems assume under value-based contracting and population health. If organizations switch to value-based care models, but don’t have the payment system to support the shift, they can’t improve the health of individuals and populations. Systems must fully understand the total cost of care and be able to look at risk contracts to ensure they’re properly paid for the services they deliver.
Under care transformation, organizations optimize care management processes and outcomes to support individuals across the continuum of care. For example, Cradle Cincinnati, an organization committed to improving infant health in the Cincinnati area, sought to address the rate of preterm births, and associated deaths and complications, in the local community. By embracing the PHM strategy of care transformation, Cradle Cincinnati identified smoking and inadequate spacing between birth as modifiable behaviors impacting preterm births (and the opportunity to save more than $25 million per year). Instead of targeting only women who were pregnant, the organization approached the continuum of pregnancy care by providing women in the community who could become pregnant with a healthy pregnancy education campaign.
Other care transformation improvement opportunities include strengthening primary care infrastructure, ensuring that appropriate care is given in the right place at the right time, and improving engagement of individuals and caregivers.
The following success stories show how health systems are actively using PHM strategies to improve outcomes:
As healthcare organizations confront a rise in at-risk contracts, they increasingly work toward the PHM goals of reducing healthcare costs and improving patient outcomes and experience. Allina Health used its analytics platform to combine several data sources, including claims data, to identify opportunities to decrease the total cost of care and improve outcomes across the care continuum.
Patients with diabetes are at a high risk for infections and substantial complications, including the risk of death from infections. Further, social determinants in these patients’ communities have a tremendous influence on their health. Texas Children’s Hospital identified gaps in diabetes care coordination in the community. With the support of an analytics platform, the hospital initiated a coordinated community response to set the standard for community management of pediatric diabetes. As a result, it improved clinician knowledge of pediatric diabetes by more than 26 percent and made individualized school packets available in the EHR to 90 percent of patients.
Unprecedented changes in the healthcare payment system are driving organizations to develop effective PHM strategies. Leading health systems are implementing data-driven care management programs to reduce healthcare costs and improve patient outcomes and experience. Data-driven care management programs that target high-risk and rising-risk patients can achieve impressive results:
With PHM strategies, organizations approach improvement from a broader continuum-care-care perspective. Instead of focusing improvement resources on limited populations and acute care, effective PHM strategies drive transformation that addresses all levels of healthcare delivery, including prevention and care management.
To begin the PHM journey and ensure that PHM strategies truly impact outcomes improvement, organizations must commit to fully understanding the PHM strategies (data, analytic, payment, and care transformation) that align with outcomes improvement and apply them to areas with the greatest opportunity for improvement.
Would you like to use or share these concepts? Download this presentation highlighting the key main points.




