Despite the widespread use of population health as a solution to control rising costs and poor outcomes, healthcare organizations struggle to effectively achieve population health success. A common barrier to success is lack of access to data about a system’s most impactable patients, their interventions, and how said interventions impact a patient’s health. However, health systems can overcome the following all-too-common population health mistakes by leveraging detailed data about their most impactable patients and interventions:
1. Lacking an effective solution for data-driven strategy.
2. Using delayed analytic insight to understand performance and opportunities.
3. Not tracking member-level data to measure intervention effectiveness.
Healthcare organizations increasingly turn to population health to deliver higher-quality care and curb today’s unsustainable healthcare spending, projected to reach $6 trillion by 2027. The industry has recognized population health as a remedy to these astronomical costs and path to improved care, allowing healthcare providers to identify their most impactable patients within their populations, quickly apply the best intervention, and improve health and outcomes across the patients the serve.
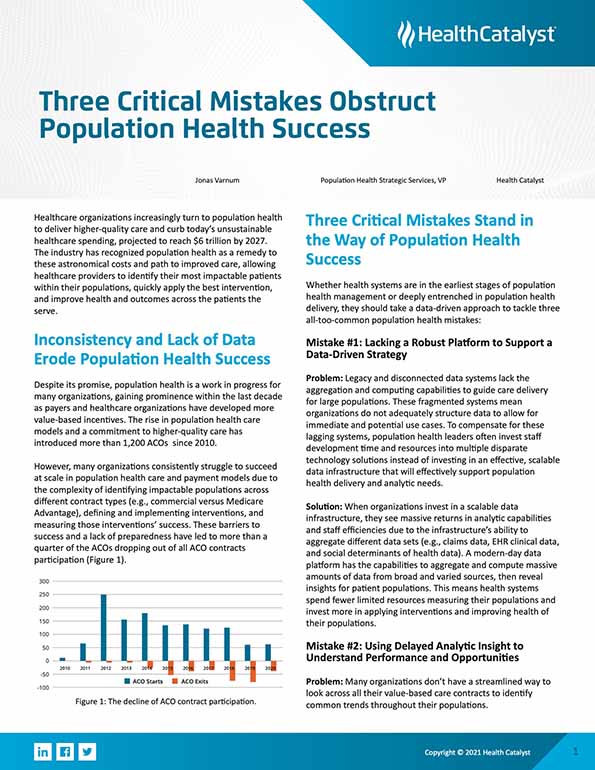
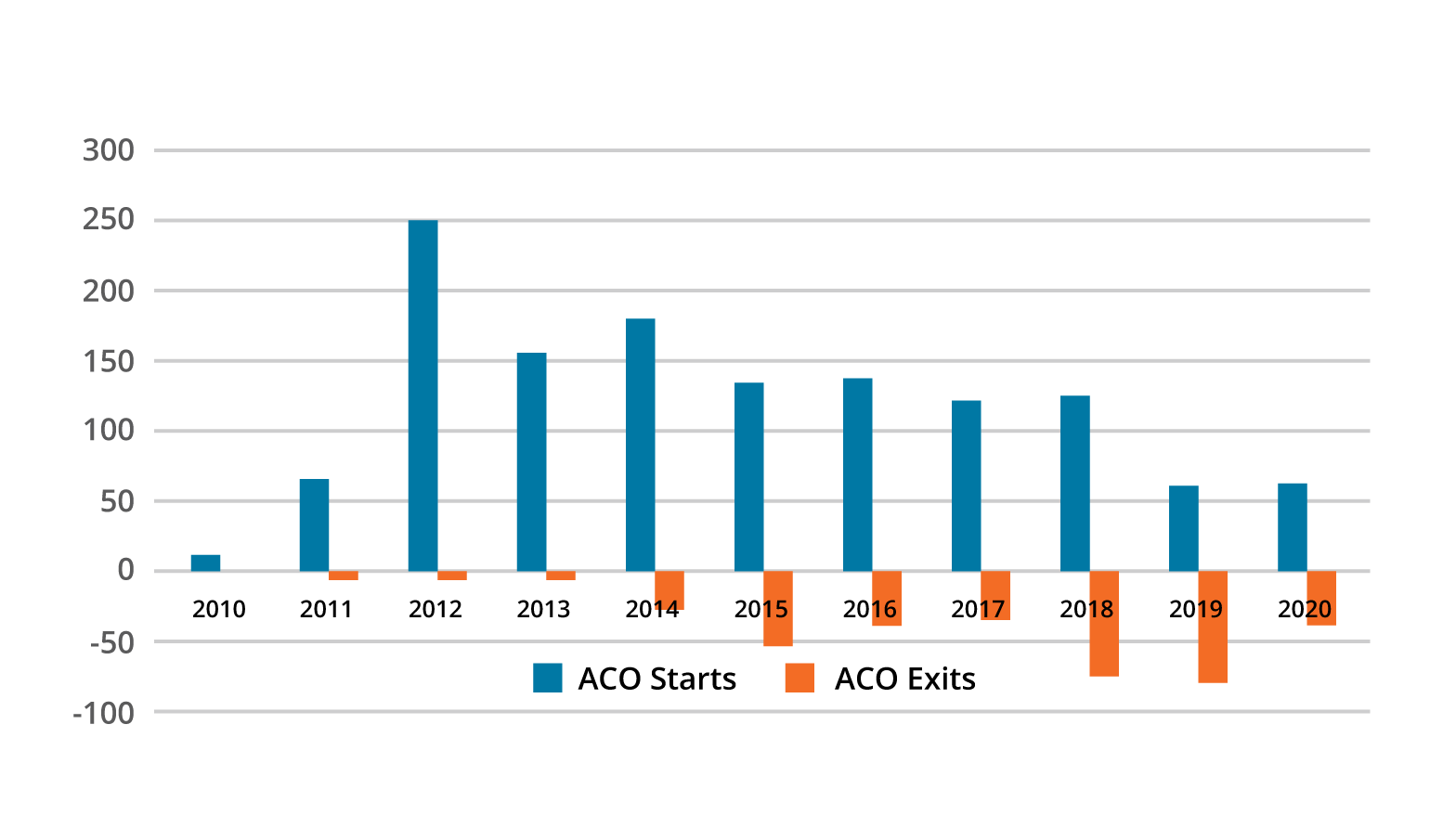
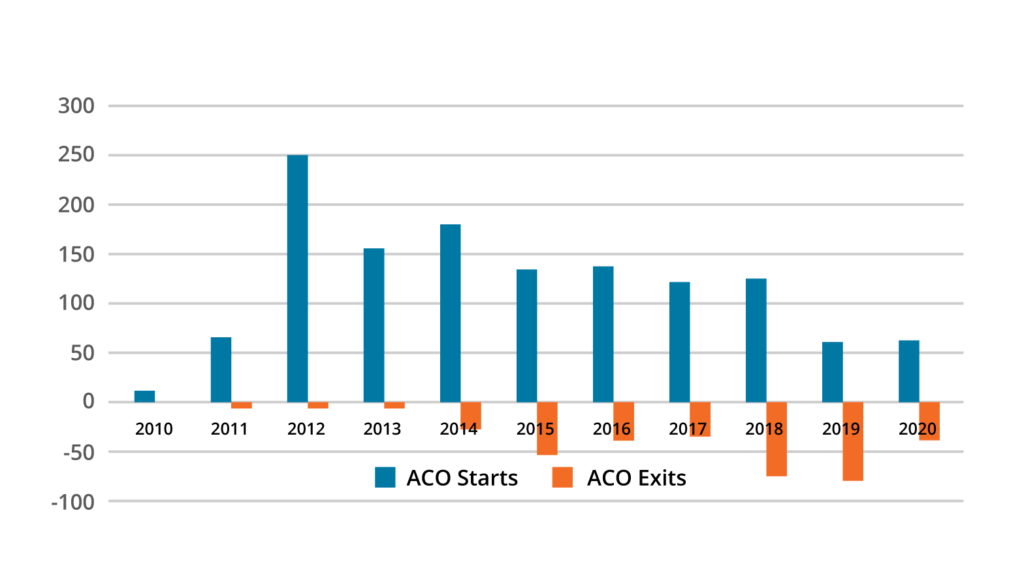
Despite its promise, population health is a work in progress for many organizations, gaining prominence within the last decade as payers and healthcare organizations have developed more value-based incentives. The rise in population health care models and a commitment to higher-quality care has introduced more than 1,200 ACOs since 2010.
However, many organizations consistently struggle to succeed at scale in population health care and payment models due to the complexity of identifying impactable populations across different contract types (e.g., commercial versus Medicare Advantage), defining and implementing interventions, and measuring those interventions’ success. These barriers to success and a lack of preparedness have led to more than a quarter of the ACOs dropping out of all ACO contracts participation (Figure 1).
Whether health systems are in the earliest stages of population health management or deeply entrenched in population health delivery, they should take a data-driven approach to tackle three all-too-common population health mistakes:
Problem: Legacy and disconnected data systems lack the aggregation and computing capabilities to guide care delivery for large populations. These fragmented systems mean organizations do not adequately structure data to allow for immediate and potential use cases. To compensate for these lagging systems, population health leaders often invest staff development time and resources into multiple disparate technology solutions instead of investing in an effective, scalable data infrastructure that will effectively support population health delivery and analytic needs.
Solution: When organizations invest in a scalable data infrastructure, they see massive returns in analytic capabilities and staff efficiencies due to the infrastructure’s ability to aggregate different data sets (e.g., claims data, EHR clinical data, and social determinants of health data). A modern-day data platform has the capabilities to aggregate and compute massive amounts of data from broad and varied sources, then reveal insights for patient populations. This means health systems spend fewer limited resources measuring their populations and invest more in applying interventions and improving health of their populations.
Problem: Many organizations don’t have a streamlined way to look across all their value-based care contracts to identify common trends throughout their populations. Historically, the process to receive and coalesce the data, then turn it into meaningful information has been time and resource intensive. However, it is critical for organizations to understand performance and compare against contracts and benchmarks to identify improvement areas so that care teams can intervene. Care teams need access to benchmarked contract performance and benchmarked patient population root cause analysis regardless of contract type.
For example, leaders need to understand their patients’ total medical spend against a variety of dimensions to understand baseline improvement opportunities. But without access to timely, actionable information, leaders can’t pinpoint and prioritize the most impactable interventions and, in some cases, rely on guesswork or anecdotal hearsay to drive decision making.
Solution: With an advanced tool, such as the Health Catalyst Value Optimizer™ solution, that instantly identifies the most valuable benchmarked opportunities for improvement across their populations’ care continuum, organizations have actionable guidance for success in risk-based contracts. For example, with timely total-cost-of-care insights drillable to a patient root-cause level (e.g., demographics, site of service, health equity status, etc.), leaders can regularly check against baselines to understand overall performance. With this insight, leaders can drill down to surface opportunities and implement the right interventions for population health success.
Problem: Effective population health requires multiple interventions. Identifying and implementing effective interventions is a complex process that could include embedding patient care gap information directly into the clinical workflow, enabling patients to utilize appropriate sites of service, or engaging with patients earlier in the care process through different access points.
In a population health care model—in which success (i.e., improving patients’ health) relies on an intervention’s success—leaders must know if, and how, their interventions impact the patients’ outcomes. And using data to track an intervention’s impact on patients’ health is the only way leaders can measure if an intervention is working and targeting its intended area. However, many organizations don’t track patient-level outcomes at a member level, usually due to lack of data capability. That is a mistake. A singular compilation of patient-level data—also known as a patient’s longitudinal record—is the only way to effectively measure an interventions’ impact on overall patient health and the overall impact on population health.
Solution: It is crucial for population health success to leverage effective interventions. For example, an integration engine that delivers analytic insight directly into the EHR workflow empowers clinicians to close patient care gaps in real time and deliver better, more cost-effective care. Embedding unfilled gaps in care directly into an EHR enables providers to easily drive outcomes, while enhancing physician satisfaction. Another intervention—providing effective care management for the right patients—requires leveraging patient-level data sets to quickly assess, intervene, and support a variety of patient populations’ diverse clinical and social needs. However, to measure an intervention’s impact and evaluate individuals at a member level, organizations must leverage a scaled, robust data engine to view organized analytic insights on their member populations. An advanced platform will also allow for quick review of underlying cost and quality outliers and the various reasons for an intervention’s impact. Organizations leveraging their comprehensive patient-level data (or longitudinal record) can more easily identify the key drivers behind an intervention’s impact over a breadth of patient utilization activities. This allows organizations to truly understand which interventions drive better patient outcomes.
For the past decade, organizations have dabbled in population health, and some have delayed its full embrace for a myriad of reasons, from existing fee-for-service contracts to a lack of executive support. Nevertheless, the longer systems wait to invest in population health, the greater the consequence for organizations and their patients.
Healthcare organizations can overcome the three common population health mistakes listed above with data-driven solutions that support high-quality data and better access for team members. These data-centric investments allow organizations to bypass much of the typical inertia impeding successful population health, allowing leaders to identify their most impactable populations, track intervention success, and ensure patients stay on the path toward optimal health.
Would you like to learn more about this topic? Here are some articles we suggest:




