The Data Operating System (DOS™) is a vast data and analytics ecosystem whose laser focus is to rapidly and efficiently improve outcomes across every healthcare domain. DOS is a cornerstone in the foundation for building the future of healthcare analytics. This white paper from Imran Qureshi details the seven capabilities of DOS that combine to unlock data for healthcare improvement:
1. Acquire
2. Organize
3. Standardize
4. Analyze
5. Deliver
6. Orchestrate
7. Extend
These seven components will reveal how DOS is a data-first system that can extract value from healthcare data and allow leadership and analytics teams to fully develop the insights necessary for health system transformation.
Population health, value-based care, decreasing revenues, and increasing costs are just a few of the pivotal issues challenging healthcare IT leaders today. Among other requirements, these issues call for large amounts of data, real-time data access, scalable analytics platforms, and systems interoperability. Healthcare IT must address all these issues, and more, even as technology becomes obsolete at an exponentially increasing pace.
Current healthcare analytics platforms are struggling because they are inflexible and don’t provide access to the right data, in the right place, at the right time to effectively support clinical, financial, and operational decision making. The current platform’s shortcomings appear in many ways: through process-driven EMRs, expensive data lakes, and unrefined transactional data.
Healthcare desperately needs a new IT model. Understanding the solution requires further investigation into a few specific IT challenges, followed by a close examination of the new model: a data-first, analytics and application platform called the Data Operating System (DOS™).
The big issues impacting healthcare, such as rising costs and decreasing margins, revolve around healthcare IT and specifically around data.
The United States is projected to spend $66 billion a year on healthcare IT by 2020. The U.S. healthcare system has spent over $34.7 billion on Meaningful Use (MU) to digitize data, yet margins are declining, physician burnout is on the rise, and patient satisfaction is low. The data produced from EMRs is plentiful, but improvement through MU is a broken promise because the data is inaccessible.
Different healthcare roles need different data for different reasons:
Though data demand is everywhere, access to the data supply remains elusive, particularly through EMRs. Clinicians often complain that they constantly put data into the EMR, but never get any data or value out. This is largely because of the current siloed and monolithic analytics environment.
The common healthcare analytics environment today looks like a series of islands (Figure 1) and navigating them is difficult.
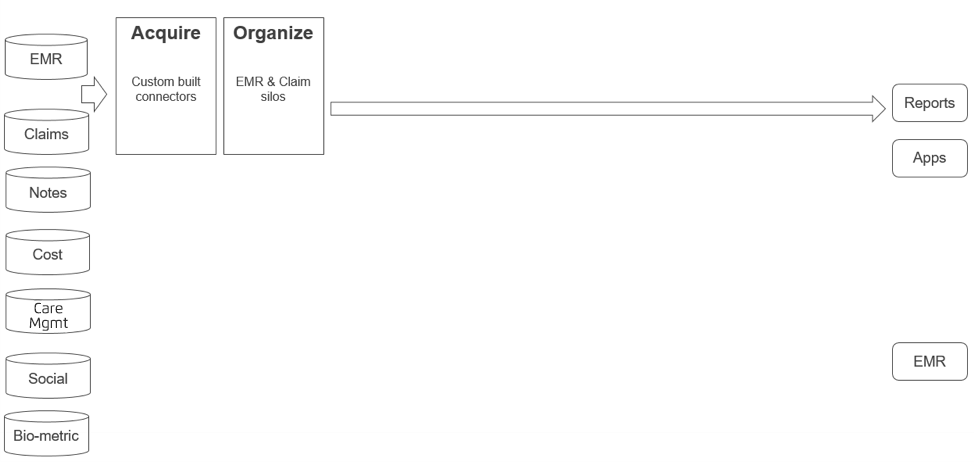
The analytics environment comprises many data sources, including EMR and claims data. Acquiring data from these sources requires custom-built connectors. Every new data source requires new understanding and another custom connector. Then the data is organized, but it still exists in silos. EMR and claims data may exist in one database or the same location, but navigation between the two data types isn’t possible (i.e., claims data isn’t accessible from the EMR record, and vice versa).
Eighty percent of the data from an EMR is unstructured, including physician notes, which hold significant value but sit completely outside the analytics system. Other data sources—social determinants of health, cost, care management, and biometric—contribute significantly to health outcomes, yet exist in silos.
In the current analytics environment, EMR and claims data is acquired and organized into reports and apps, but this is where content and logic can get confusing. For example, when determining a cohort of patients with diabetes, individual reports may use different logic to define which ICD-10 codes constitute diabetes.
Further complicating the environment is an isolated EMR, which is entirely separate from the analytics infrastructure. It is very hard to get insights generated by the analytics infrastructure in front of clinicians at the point of care.
The entire system is monolithic—users cannot customize it with components and they are predestined to a single configuration.
The current analytics model is the lockbox around healthcare data and the key to unlock it is DOS.
DOS is a new data-first analytics and applications platform. Before we talk about the mechanics of DOS, it helps to understand the idea of “data first” and why EMRs cannot trace a data-first trajectory. Then high-level and magnified diagrams will help explain DOS structure and components, and the purpose of each piece in the system.
Processes have driven the current healthcare data environment. The requirement to digitize medical records has spurred massive EMR deployment. EMRs are process-first systems, designed to move data from person to person to follow a process. EMRs collect data within a specific workflow, but don’t allow access to, or the import of, data outside this workflow, making it very difficult to do any meaningful analytics on transactional data. Like mainframe computers, EMRs will always be necessary, but they are not the right tool for unlocking data.
To extract value from the healthcare data, we need a data-first approach. In data-first systems, the focus is on the following:
The iPhone is a good example of a data-first environment. Various applications built into the iPhone receive data and enter it into the ecosystem in different ways:
Other applications consume this data, create insights, then publish those insights into the ecosystem, where they can be picked up by yet another application. In a data-first environment like DOS, data drives the process. Instead of implementing a process and moving data from place to place (like an EMR), data is analyzed and the analysis drives the process.
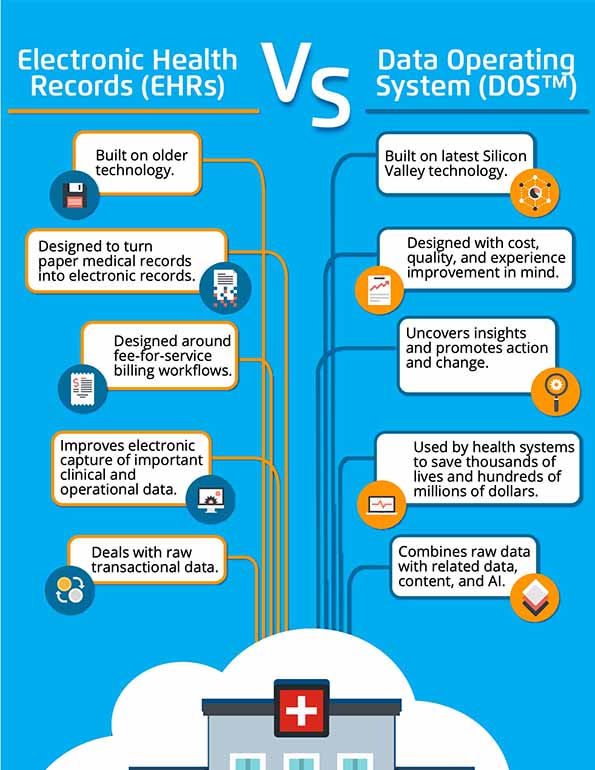
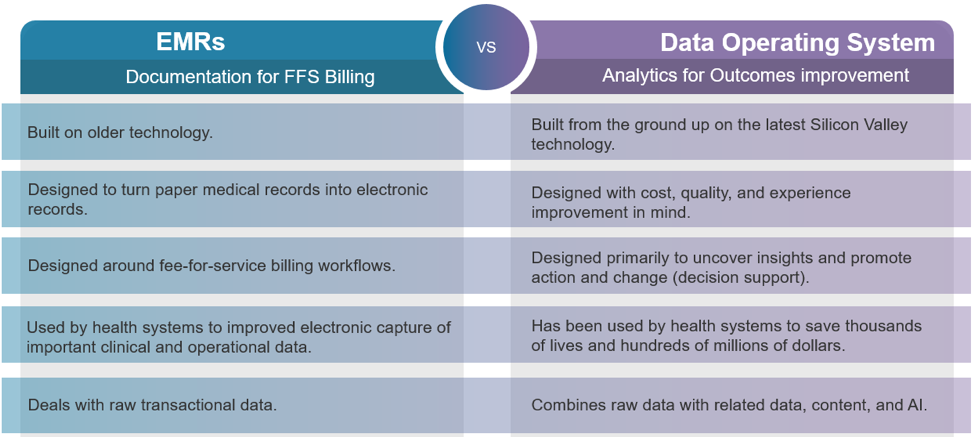
EMRs were designed to produce documentation for fee-for-service (FFS) billing, which is their fundamental purpose. DOS is designed for analytics and outcomes improvement. The core of EMRs and the core of DOS differ in five other key areas (Figure 2).
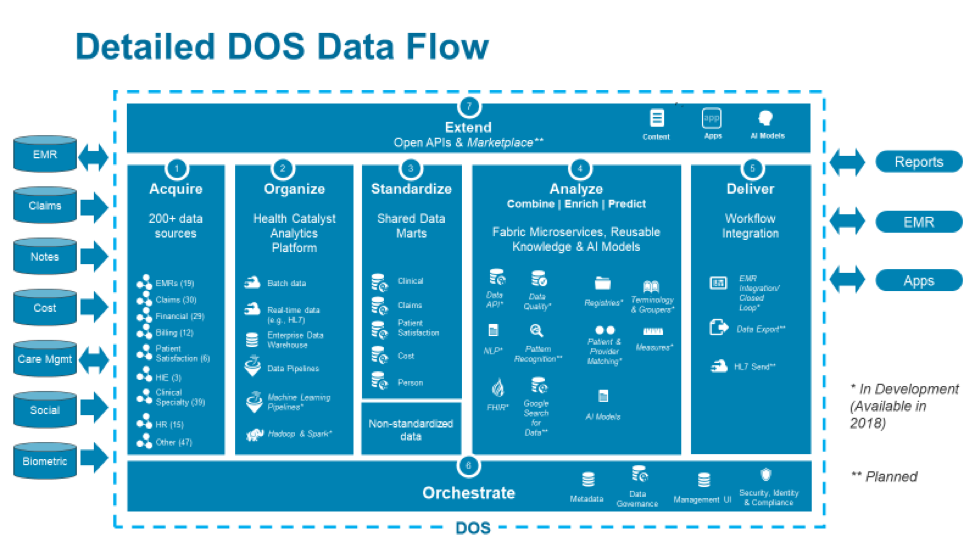
Like the current analytics environment, DOS interacts with multiple data sources, reports, apps, and EMRs. The unique and comprehensive structure, missing from the current model, lives in between these elements. This structure transforms data so reports and apps don’t have to, and it includes seven components.
1. Acquire
Healthcare analytics systems need data from many sources, so the cost of acquiring data from any data source needs to be low. DOS builds in connections to more than 200 data sources, including most of the common healthcare data.
2. Organize
The Health Catalyst® Analytics Platform is the organizing function of DOS. It includes all the tools to rapidly consolidate data from every source, precluding the need to custom build anything. Data analysts can create data pipelines to transform data through multiple steps, then leverage data lakes, and Hadoop and Spark infrastructures to process large amounts of data through the system.
3. Standardize
After it’s organized, clinical data (e.g., patient populations, diagnosis classifications, medication groupings) can be efficiently standardized through pre-built shared data marts. These can be used out of the box, or users can create their own from built-in tooling.
4. Analyze
Using data and content microservices, the analyze component combines and enriches data, then makes predictions using AI models. This is the process of converting raw data to deep data.
5. Deliver
Once data is analyzed, DOS can deliver it directly to the EMR workflow and right to clinicians’ fingertips. Data can also be exported to other workflows, putting it where data analysts are, rather than making them navigate to the data. DOS learns through a closed-loop function. As analysts interact with the system, those interactions feed back into the system and improve the data over time.
6. Orchestrate
Orchestrating all this data requires a central place for storing metadata (i.e., data about data), so people can easily find and understand the data. Orchestration also requires a central place for enforcing security, and a central place to manage the various processes happening in the analytical environment. DOS provides these tools so anyone can find, manage, and secure all the organization’s data.
7. Extend
All the pieces of DOS are accessible through open APIs to ensure sustainability of the DOS environment. A marketplace allows users to choose different applications and content pieces for their own data operating system.
This is the high-level view of DOS. The following section will zoom into the operating system for greater scrutiny of each component.
What does DOS offer, through each of the seven components, that really helps jumpstart a healthcare system’s analytical efforts? A deeper examination reveals DOS’s full capabilities (Figure 3).
DOS builds in connectors to more than 200 data sources (Figure 4), including all the common EMRs, most claims systems, financial systems, billing systems, HIEs, and clinical and patient satisfaction systems.
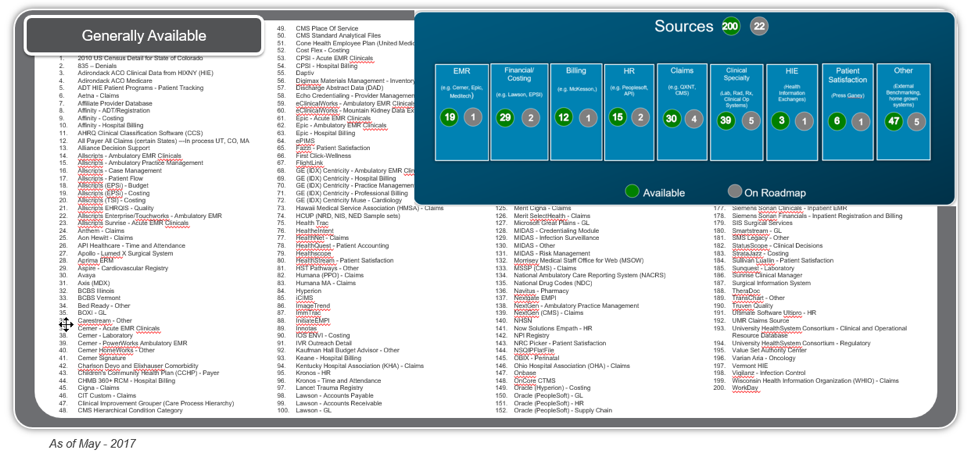
It takes very little effort to bring in data from these systems. DOS already understands them, can map to them appropriately, and can serve up the data for analysis.
To understand the value of this DOS component, consider how data lakes and data warehouses have been developed and deployed (Figure 5).
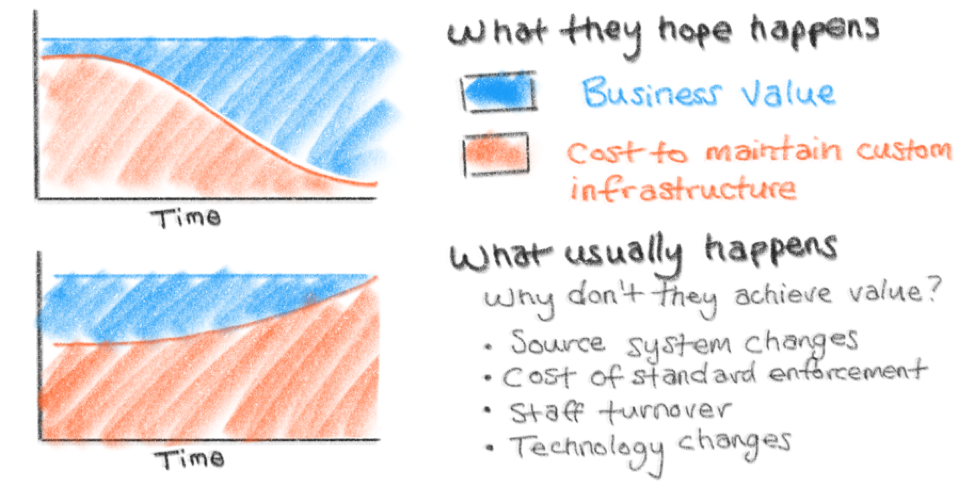
At the outset, the hope is that, over time, the business value of the data lake or warehouse will increase as the costs to maintain it decrease. What ends up happening is almost the exact opposite. Source systems change. An EMR is upgraded. The warehouse needs to pull data from a new claim source. These all incur substantial costs. After a while, staff turnover interrupts continuity, then the underlying technology changes, the data warehouse can’t keep up and, as a result, people stop using it.
DOS delivers the desired value-to-cost curve, with value increasing and costs decreasing over time (Figure 6).
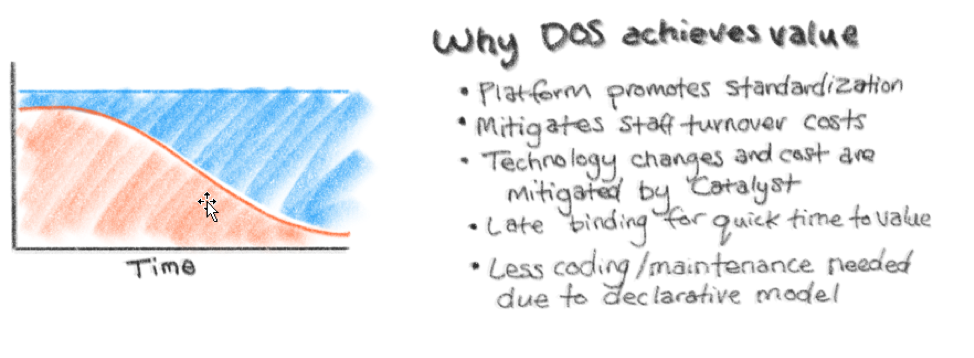
DOS starts with all the necessary building blocks, so there’s less programming involved. Much of the data organizing function is performed by DOS “under the hood.” As new staff comes on board, they can use DOS’s built-in tools (UI and other simple models) to manage and enhance the existing functionality rather than looking through piles of handwritten scripts.
Health Catalyst manages technology changes, so healthcare systems can focus on deriving business value from the data warehouse. The Late-Binding™ technology in DOS binds only the data that’s needed immediately, which generates very fast time-to-value. More data can be added over time. It’s not necessary to create a dimensional model of all the data up front, a process that usually takes years before any value is derived from it.
DOS standardizes data through shared data marts (Figure 7), but there’s a cost to doing this, so pursue standardization only when there’s agreement on the interpretation of that data and when standardization adds value. For example, standardizing the ICD-10 codes classified as diabetes likely makes sense, but creating a grouping for medications that are only ever used by one department may not be worth it.
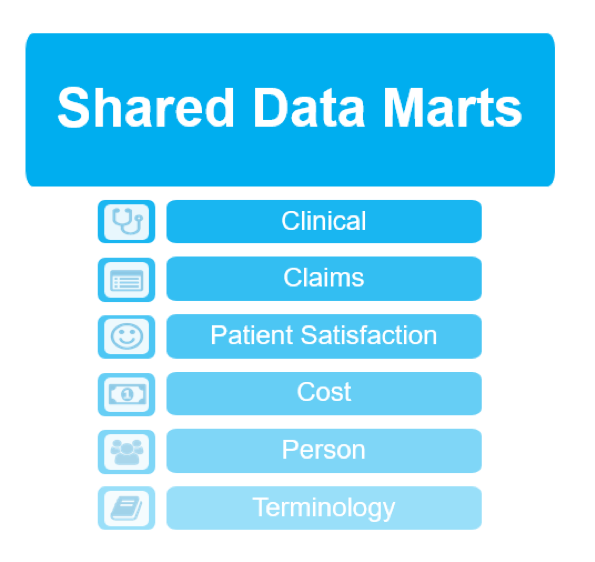
Standardizing data creates faster time-to-value and allows for building multiple reports and applications without having to create multiple mappings of the same data. Standardizing creates tighter data governance through controlled data access and data definitions.
DOS has built-in shared data marts around clinical, claims, patient satisfaction, cost, person, and terminology. DOS takes the 200+ data sources mentioned earlier and maps them into these shared data marts, giving access to data that’s aggregated across every data mart. This mapping effectively disintegrates silos by joining clinical and business data from multiple EMR systems and other data sources, such as claims, GL, and patient satisfaction.
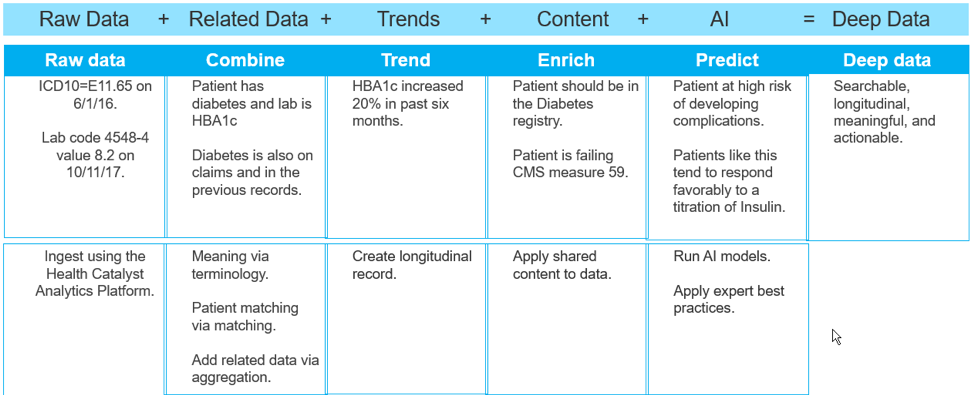
The term big data refers to data in terms of volume, variety, and velocity. But the IT vernacular has introduced a new term, deep data, which is about understanding data. The analyze component of DOS transforms raw data into deep data through five steps:
Figure 8 shows an example of transforming raw data (from a single patient with diabetes) into deep data that predicts risks and suggests interventions.
DOS’s delivery component gets the right data to the right place at the right time. The EMR’s current model for clinical decision support (CDS) is interruptive. Pop-ups serve as alerts, but don’t provide any underlying data so clinicians can understand the reasons behind the alerts. And there’s no way to correct a misleading alert. DOS delivery focuses on synthesizing data, so clinicians can choose the right path, rather than conforming to an A or B approach.
The model for CDS in DOS is like the Google Maps model. Google Maps shows a recommended route, but also displays alternate routes and travel times. The user can click any route, even if it’s not the fastest or shortest one. The app color codes routes, which helps explain why one route is recommended over another. Users get the benefits of Google Maps, but can still direct it according to their preferences.
This CDS model is built into DOS, as is the technology that can show previously created data and insights directly within existing workflows. Figure 9 shows a sample record of a patient at high risk of opioid abuse. It displays the patient’s risk factors, history, and suggested interventions (actions): all relevant insights for the attending clinician. Any actions are directed back into the workflow of the EMR, keeping all documentation internal. This augments the EMR and delivers the power of deep data and insights to the clinician’s fingertips.

What’s the value of data if analysts can’t find what they are looking for or can’t understand where the data came from? Many organizations try to build their own orchestration tools but end up spending a significant amount of time on these tools instead of focusing on getting business value. DOS provides orchestration tools around creating and managing metadata, enforcing security, and managing all the analytical processes.
DOS can be extended through open APIs and a marketplace of content, apps, and AI models. This extend component allows customization for every healthcare enterprise.
APIs are important because they accelerate app development. With APIs, developers can customize existing tools and services to build only what they need. DOS ensures that everything that needs to be built is done so within the operating system and connected by an API fabric.
Several fabric APIs are already available in DOS:
Three fabric APIs are in development:
A huge value of DOS is its ability to learn from data within a closed-loop system. After clinicians receive data, there’s the possibility they won’t agree with it or that the data is non-responsive (i.e., it’s read-only data). Data should be alive (i.e., read-write) and be able to transmit insights across the care spectrum. This is what happens in a closed-loop system (Figure 10).
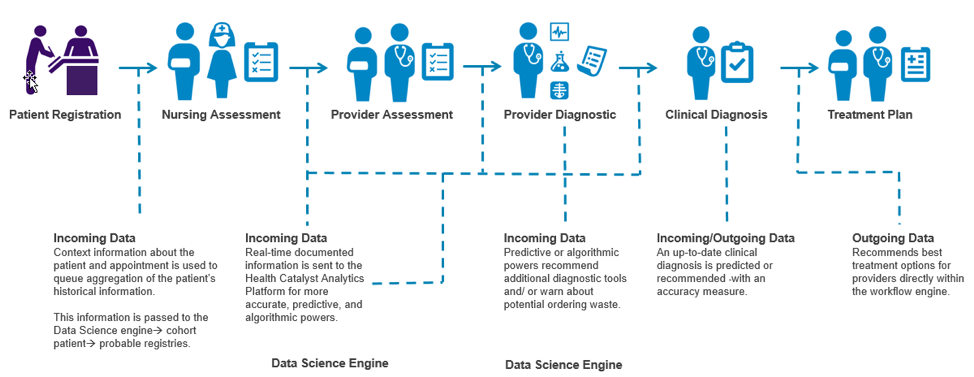
In the example shown in Figure 10, data is generated when a patient registers. This data is analyzed to see what stands out in the patient’s history. As clinicians make assessments, the patient is assigned to appropriate cohorts and registries. This data feeds back into the system in real time, which continues to update insights even as additional diagnoses feed into the system in real time. Risk predictions determine additional diagnoses or interventions, which are then presented as part of the treatment plan. This process involves different clinicians who interact with the data; the closed loop keeps bringing all the information back around so the data changes and improves over time.
Data consumers want their data sooner than the next day, but faster turnaround has been next to impossible. Real-time data processing follows a complex pathway that must receive messages, process them asynchronously, establish data reliability, and map the data from HL7 to a database (Figure 11).
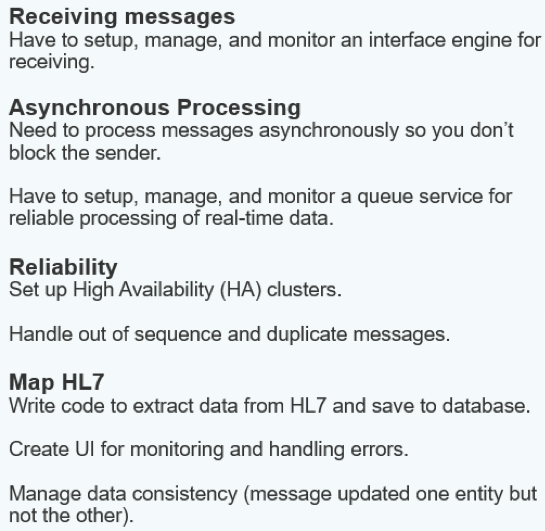
Real-time data processing is vital to healthcare, but too difficult for healthcare systems to develop on their own. DOS provides a four-step real-time processing solution:
Installing an interface engine isn’t necessary; all the asynchronous processing is built in. High availability and deduplication are built in. Data is already converted to XML, so it is easy for applications to consume. Applications can subscribe to the queue server and receive processed messages in real time too.
DOS is a complete analytics ecosystem that has seven key attributes:
DOS’s attributes generate many benefits that impact leaders throughout the healthcare organization:
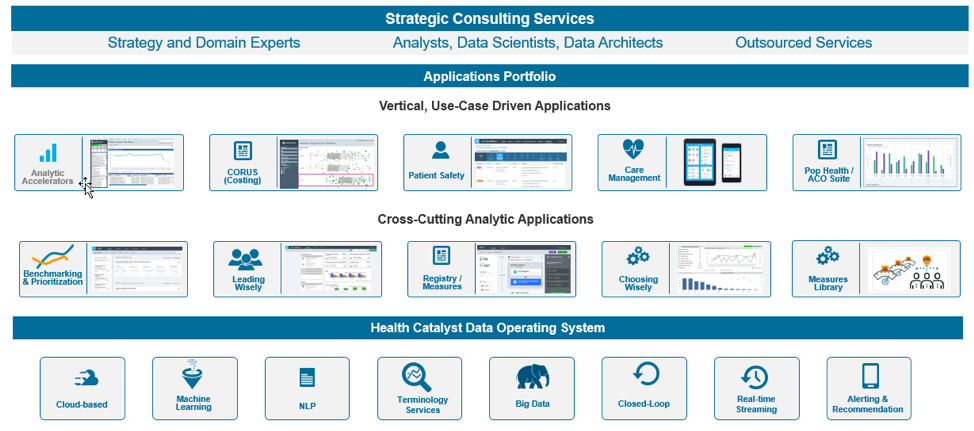
DOS enables many applications and services, which sit on top of the operating system (Figure 12). Several cross-cutting analytic applications and vertical, use-case driven applications facilitate many healthcare programs. Health Catalyst builds some of these applications, but third parties can also build their own applications. In addition, Health Catalyst provides a line of strategic consulting services to implement the technologies and ongoing operating system improvements.
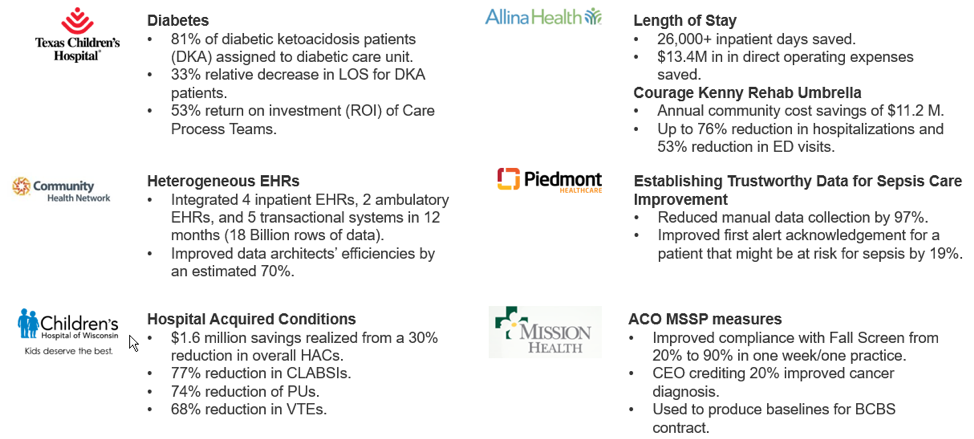
Components built over the last decade, and now available in DOS, have shown value in millions of dollars saved through process and outcomes improvement (Figure 13).
Healthcare needs a new IT model to accommodate a rapidly evolving data landscape. EMRs, raw transactional data, and data lakes are useful, but no longer sufficient. The DOS approach is the only way to unlock healthcare data.
DOS easily acquires data from more than 200 data sources, organizes it with a built-in analytics platform, leverages standard and custom data models, accepts real-time data, and brings report logic into a common layer. DOS conveys data to the EMR and other workflow tools so clinicians can act on it. The closed-loop system keeps the data live and updated, and APIs extend the operating system.
Leaders across the healthcare enterprise can benefit from DOS. DOS also benefits independent software vendors, giving them access to clinical data through built-in APIs, so they can easily integrate data into clinical workflows.
Despite its huge scope and vast capabilities, DOS can get up and running quickly, delivering value within just a few months. DOS is a foundational and transformational system that has the potential to change the healthcare economy and massively improve financial, clinical, and operational outcomes.
Would you like to use or share these concepts? Download this presentation highlighting the key main points.




